Book Appoinment
Leukaemia
Leukemia starts when the DNA of a single cell in your bone marrow changes (mutates) and can’t develop and function normally. Leukemia cells often behave like abnormal white blood cells. Treatments for leukemia depend on the type of leukemia you have, your age and overall health, and if the leukemia has spread to other organs or tissues.
Overview
What is leukemia?
Leukemia is a cancer of the blood, characterized by the rapid growth of abnormal blood cells. This uncontrolled growth takes place in your bone marrow, where most of your body’s blood is made. Leukemia cells are usually immature (still developing) white blood cells. The term leukemia comes from the Greek words for “white” (leukos) and “blood” (haima).
Unlike other cancers, leukemia doesn’t generally form a mass (tumor) that shows up in imaging tests, such as X-rays or CT scans.
There are many types of leukemia. Some are more common in children, while others are more common in adults. Treatment depends on the type of leukemia and other factors.
How does leukemia develop?
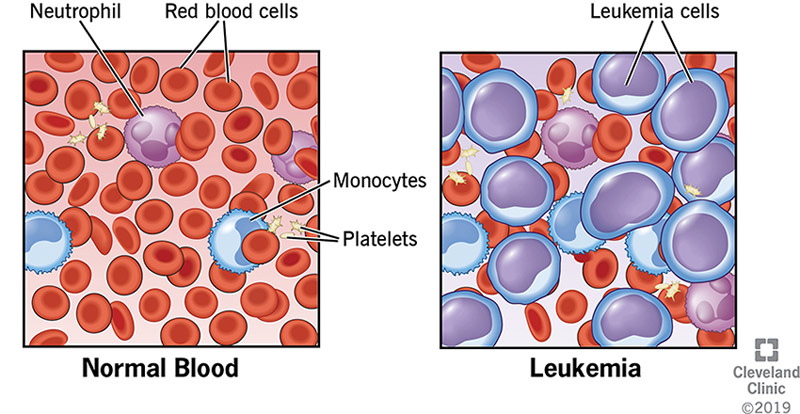
Leukemia begins in bone marrow, the soft spongy tissue in the inner cavity of your bones, where your body’s blood cells are made. Blood cells go through multiple stages before reaching their fully mature forms. Mature, normal blood cells include:
- Red blood cells: Cells that carry oxygen and other vital materials to all tissues and organs in your body.
- White blood cells: Cells that fight infection.
- Platelets: Cells that help your blood clot.
These blood cells start as hematopoietic (hemo = blood, poiesis = make) stem cells. The stem cells develop into either myeloid (MAI-uh-loyd) cells or lymphoid (LIM-foyd) cells. If blood cells were to continue to develop normally, the mature forms of these cells are as follows:
- Myeloid cells Cells that carry oxygen and other vital materials to all tissues and organs in your body.
- Lymphoid cells develop into certain white blood cells (lymphocytes and natural killer cells).
However, if you have leukemia, one of the developing blood cells begins to multiply out of control. These abnormal cells — called leukemia cells — begin to take over the space inside of your bone marrow. They crowd out the cells trying to develop into healthy red blood cells, white blood cells and platelets.
How does leukemia affect my body?
Having too many leukemia cells and too few normal cells is harmful for several reasons:
- Leukemia cells serve no purpose in keeping you healthy.
- Normal blood cells have very little space and support to mature and multiply inside of your bone marrow because the leukemia cells overtake them.
What are the different types of leukemia?
There are four main types of leukemia and several subtypes. Healthcare providers classify leukemia based on how fast the disease worsens and whether leukemia cells arise from myeloid cells or lymphoid cells.
Classifications of leukemia
Healthcare providers classify leukemia based on how quickly it progresses and the type of blood cell involved.
By speed of disease progression
- Acute leukemia. The leukemia cells divide rapidly and the disease progresses quickly. If you have acute leukemia, you’ll feel sick within weeks of the leukemia cells forming. Acute leukemia is life-threatening and requires immediate initiation of therapy. Acute leukemia is the most common cancer in children.
- Chronic leukemia. Often, these leukemia cells behave as both immature and mature blood cells. Some cells develop to the point where they function as the cells they were meant to become — but not to the extent their normal counterparts do. The disease typically worsens slowly compared to acute leukemia. If you have chronic leukemia, you may not have noticeable symptoms for years. Chronic leukemia is more common in adults than in children.
By cell type
- Myelogenous (mai-uh-lOW-juh-nuhs) or myeloid leukemia develops from myeloid cells. Normal myeloid cells develop into red blood cells, white blood cells and platelets.
- Lymphocytic leukemia develops from lymphoid cells. Normal lymphoid cells develop into white blood cells that are an important part of your body’s immune system.
Types of leukemia
There are four main types of leukemia:
- Acute lymphocytic leukemia (ALL) is the most common type of leukemia in children, teens and young adults up to age 39. ALL can affect adults of any age.
- Acute myelogenous leukemia (AML) is the most common type of acute leukemia in adults. It’s more common in older adults (those over 65). AML also occurs in children.
- Chronic lymphocytic leukemia (CLL) is the most common chronic leukemia in adults (most common in people over 65). Symptoms may not appear for several years with CLL.
- Chronic myelogenous leukemia (CML) is more common in older adults (most common in people over 65) but can affect adults of any age. It rarely occurs in children. Symptoms may not appear for several years with CML.
How common is leukemia?
Leukemia is the 10th most common cancer in the U.S., accounting for 3.2% of all new cancer cases. Leukemia can affect anyone, but it’s more common among people who are:
- Ages 65 to 74.
- Assigned male at birth (AMAB).
- Caucasian/white.
Many people think of leukemia as a pediatric cancer, but some forms develop more often in adults. Although leukemia is rare in children, it’s the most common form of cancer affecting children and teens.
Symptoms and Causes
What are the symptoms of leukemia?
Symptoms depend, in part, on the type of leukemia. For instance, if you have a chronic form of leukemia, you may not have noticeable symptoms in the early stages.
Common signs and symptoms of leukemia include:
- Fatigue, tiring easily.
- Fever or night sweats.
- Frequent infections.
- Shortness of breath.
- Pale skin.
- Unexplained weight loss.
- Bone/joint pain or tenderness.
- Pain or full feeling under your ribs on the left side
- Swollen lymph nodes in your neck, underarm, groin or stomach, an enlarged spleen or liver.
- Bruising and bleeding easily, including nosebleeds, bleeding gums, a rash that looks like tiny red spots in skin (petechiae) or purplish/darkened skin patches.
What causes leukemia?
Leukemia starts when the DNA of a single cell in your bone marrow changes (mutates). DNA is the “instruction code” that tells a cell when to grow, how to develop and when to die. Because of the mutation, or coding error, leukemia cells keep multiplying. All cells arising from the original mutated cell also have the mutated DNA.
Scientists don’t know what causes these developing cells to mutate. They’ve been able to identify some common mutations that people diagnosed with different types of leukemia share.
Are certain people at a higher risk for developing leukemia?
Anyone can develop leukemia. Still, studies have shown that certain factors may increase your risk, including:
- Previous cancer treatment. Past cancer treatments involving radiation or chemotherapy may increase the likelihood you’ll develop some types of leukemia.
- Smoking. If you have a history of smoking or exposure to second-hand smoke, you’re at increased risk of developing acute myelogenous leukemia.
- Exposure to industrial chemicals.Benzene and formaldehyde are known cancer-causing chemicals found in building materials and household chemicals. Benzene is used to make plastics, rubbers, dyes, pesticides, drugs and detergents. Formaldehyde is in building materials and household products such as soaps, shampoos and cleaning products.
- Certain genetic disorders.Genetic disorders, such as neurofibromatosis, Klinefelter syndrome, Schwachman-Diamond syndrome and Down syndrome, may increase your risk.
- Family history of leukemia.Research suggests that some types of leukemia may run in families. In most cases, however, having a relative with leukemia doesn’t mean that you or another family member will also develop leukemia. Tell your healthcare provider if you or a family member has a genetic condition. They may recommend genetic testing to assess your risk.
Diagnosis and Tests
How is leukemia diagnosed?
Results from routine blood work can alert your healthcare provider that you may have an acute or chronic form of leukemia that requires further testing. Or they may recommend a workup if you have leukemia symptoms.
Diagnostic exams and tests may include:
- Physical exam: Your healthcare provider will ask about your symptoms and feel for swollen lymph nodes and an enlarged spleen or liver. They may also inspect your gums for bleeding and swelling. They may look for a skin rash associated with leukemia that may appear red, purple or brown.
- Complete blood count (CBC): This blood test lets your healthcare provider know if you have abnormal levels of red blood cells, white blood cells and platelets. If you have leukemia, you’ll likely have higher than normal counts of white blood cells.
- Blood cell examination: Your healthcare provider may take additional blood samples to check for markers that indicate the presence of leukemia cells or a specific type of leukemia. Flow cytometry and peripheral blood smear are additional tests your healthcare provider may order.
- Bone marrow biopsy (bone marrow aspiration): Your healthcare provider may perform a biopsy if you have an abnormal white blood cell count. A long needle inserted into your bone marrow (usually in your pelvic bone) draws out fluid during the procedure. The fluid sample gets tested in a lab for leukemia cells. A bone marrow biopsy helps determine the percentage of abnormal cells in your bone marrow, confirming a leukemia diagnosis.
- Imaging and other tests: Your doctor may order a chest X-ray, CT scan, or magnetic resonance imaging (MRI) scan if symptoms indicate leukemia has affected your bones, organs or tissue. The leukemia cells don’t show up on imaging.
- Lumbar puncture (spinal tap): Your healthcare provider may test a sample of spinal fluid to see if leukemia has spread to the spinal fluid surrounding your brain and spinal cord.
Management and Treatment
How is leukemia treated?
Treatments for leukemia depend on the type of leukemia you have, your age and overall health, and if the leukemia has spread to other organs or tissues.
Common treatments often include a combination of the following:
- Chemotherapy: Chemotherapy is the most common form of leukemia treatment. It involves using chemicals to kill leukemia cells or keep them from multiplying. During treatment, you may receive the chemicals (medication) as a pill, an injection into a vein or a shot under your skin. Usually, you’ll receive a combination of chemotherapy drugs.
- Immunotherapy (biologic therapy):This treatment uses certain drugs to boost your body’s defense system — your immune system — to fight leukemia. Immunotherapy helps your immune system identify cancer cells and produce more immune cells to fight them.
- Targeted therapy:This treatment uses drugs designed to attack specific parts of a leukemia cell (like a protein or gene) that are causing them to overtake normal blood cells. Targeted therapies may prevent leukemia cells from multiplying, cut off the cells’ blood supply or kill them directly. Targeted therapy is less likely to harm normal cells. Examples of targeted therapy drugs include monoclonal antibodies and tyrosine kinase inhibitors.
- Radiation therapy: This treatment uses strong energy beams or X-rays to kill leukemia cells or stop them from growing. During treatment, a machine directs radiation to the exact spots in your body where the cancer cells are or distributes radiation over your whole body. Distributing radiation throughout your body may happen before a hematopoietic cell transplant.
- Hematopoietic cell transplant (stem cell or bone marrow transplant): This treatment replaces the cancerous blood-forming cells killed by chemotherapy and/or radiation therapy with new, healthy hematopoietic cells. Your healthcare provider may remove these healthy cells from your blood or bone marrow before chemo and radiation, or they may come from a donor. The healthy new cells multiply, forming new bone marrow and blood cells that become the red blood cells, white blood cells and platelets your body needs.
- Chimeric antigen receptor (CAR) T-cell therapy: This is a novel type of therapy that takes your body’s infection-fighting T-cells (T-cell or T-lymphocyte is a type of immune cell), engineers them to fight leukemia cells and infuse them back into your body.
Clinical trials are also available to test new cancer treatments. Weigh the potential benefits and risks of enrolling in a clinical trial with your healthcare provider.
What are the phases of leukemia treatment?
Depending on your treatment plan, you may receive ongoing leukemia treatments long-term or treatment in phases. Generally, phased treatment involves three parts. Each phase has a specific goal.
- Induction therapy The goal is to kill as many leukemia cells as possible in your blood and bone marrow to achieve remission. In remission, blood cell counts return to normal levels, no leukemia cells are found in your blood, and all signs and symptoms of the disease disappear. Induction therapy usually lasts four to six weeks.
- Consolidation (also called intensification). The goal is to kill any remaining undetected leukemia cells, so the cancer doesn’t return. You’ll usually receive consolidation therapy in cycles, over four to six months.
- Maintenance therapy. The goal is to kill any leukemia cells that may have survived the first two treatment phases and prevent the cancer from returning (relapse). Treatment lasts about two years.
Your healthcare provider may resume or change your treatment if the leukemia returns.
Outlook / Prognosis
What outcome can I expect if I have a leukemia diagnosis?
It’s difficult to predict the prognosis for leukemia because everyone’s experience is different. Outcomes depend on a variety of factors, including:
- Genetic abnormalities or mutations. The mutations inside leukemia cells are the most important predictor of outcome.
- Type of leukemia. Certain types of leukemia are associated with more favorable outcomes than others.
- Blood cell counts at the time of diagnosis. The number of leukemia cells at your diagnosis can play a role in your outcome.
- Age. Generally, the younger you are at your diagnosis, the better your outcome.
- Health. Generally, the healthier you are at your diagnosis, the better your outcome.
- Response to treatment. The length of time it takes for cancer to go into remission often indicates how successful treatment may be.
- Presence of leukemia cells in your central nervous system. Cells in your spinal fluid are often more difficult to treat.
Ultimately, your healthcare provider is the most reliable resource for understanding how your cancer affects your unique prognosis. Ask them about treatment outcomes.
What is the survival rate of leukemia?
Although the number of new cases of leukemia in the U.S. has remained relatively steady or slightly increased since the 1970s, the survival rate has also improved. Still, long-term outcomes vary for each person.
The National Cancer Institute reports the following survival data for the four main types of leukemia:
| Types of Leukemia | ALL | AML | CLL | CML |
|---|---|---|---|---|
| 5-year survival rate* | 69.9% | 29.5% | 87.2% | 70.6% |
| Number of deaths per 100,000 persons | 0.4 | 2.7 | 1.1 | 0.3 |
| Death is highest among those aged | 65-84 | 65+ | 75+ | 75+ |
Table legend:
ALL = acute lymphocytic leukemia; AML = acute myelogenous leukemia; CLL = chronic lymphocytic leukemia; CML = chronic myelogenous leukemia
*survival compares patients diagnosed with cancer vs. people of same age, race and sex who are cancer free.
Data source: SEER Cancer Statistics Review, 1975-2017, National Cancer Institute. Bethesda, MD.
Can leukemia be cured?
There isn’t a cure for leukemia, but this doesn’t mean some people don’t achieve long-term remission. Being cured of leukemia means that the cancer’s gone, it’s not coming back and no more treatment is needed — but this is hard to know for sure with leukemia.
On the other hand, long-term remission means there’s no sign of cancer with or without treatment. Remission may last anywhere from a few weeks to many years. The leukemia may never return. If it does, your healthcare provider may recommend new treatments to achieve remission.
Your healthcare team can best answer the question, “Am I cured of my leukemia?” Your team will work closely with you to monitor your health and develop a personalized treatment plan.
Living With
What questions should I ask my provider?
Empower yourself by learning all you can about how your cancer diagnosis may uniquely impact you. It’s a good idea to take notes and bring a friend to your appointments. Don’t be afraid to ask questions.
Questions may include:
- What type of leukemia do I have? In what type of cell? Is it a fast- or slow-growing kind of cancer?
- How early was the leukemia discovered?
- What are my treatment options?
- What are the benefits and risks of each type of treatment?
- What treatment plan is best suited for me? Why?
- When should treatment begin?
- How long will treatment (and each stage of treatment) last?
- How long will I be in the hospital?
- What are the side effects of treatment? What can be done to prevent or lessen these side effects?
- What if I want to have children? What are my options for preserving my fertility?
- What’s the success rate/survival rate for my type of leukemia?
- Should I enroll in a clinical trial?
Additional Common Questions
Where can I find clinical trials for leukemia?
To learn more about clinical trials for leukemia, visit:
- Leukemia & Lymphoma Society Clinical Trial Support Center.
- National Cancer Institute: Clinical Trials Information for Patients and Caregivers.
- American Cancer Society: Clinical Trials.
- Cancer Trials at Cleveland Clinic.
Where can I find support groups?
To connect with people with leukemia or to locate additional support from people who understand what it means to live with a cancer diagnosis, visit your local Leukemia & Lymphoma Society chapter.
A note from Cleveland Clinic
Any cancer diagnosis is scary, but a leukemia diagnosis may feel especially so. It can be difficult to imagine what the treatment experience will be like without a tumor that can be removed. It can be intimidating to imagine the prognosis. Remember that leukemia isn’t one thing with one outcome. Your treatment and your chance of long-term remission depend on many factors. No one can predict your outcomes without understanding your health and leukemia — down to the characteristics of the leukemia cells. Talk with your healthcare provider about what a leukemia diagnosis means for you.