Book Appoinment
Bile Duct Cancer
Cholangiocarcinoma (bile duct cancer) is a rare, aggressive form of cancer. It often affects adults in their 70s and has spread beyond the bile ducts by the time healthcare providers diagnose it. Treatment usually involves a combination of surgery, chemotherapy or radiation therapy. Clinical trials to improve the outcomes of cholangiocarcinoma are ongoing.
Overview
What is cholangiocarcinoma (bile duct cancer)?
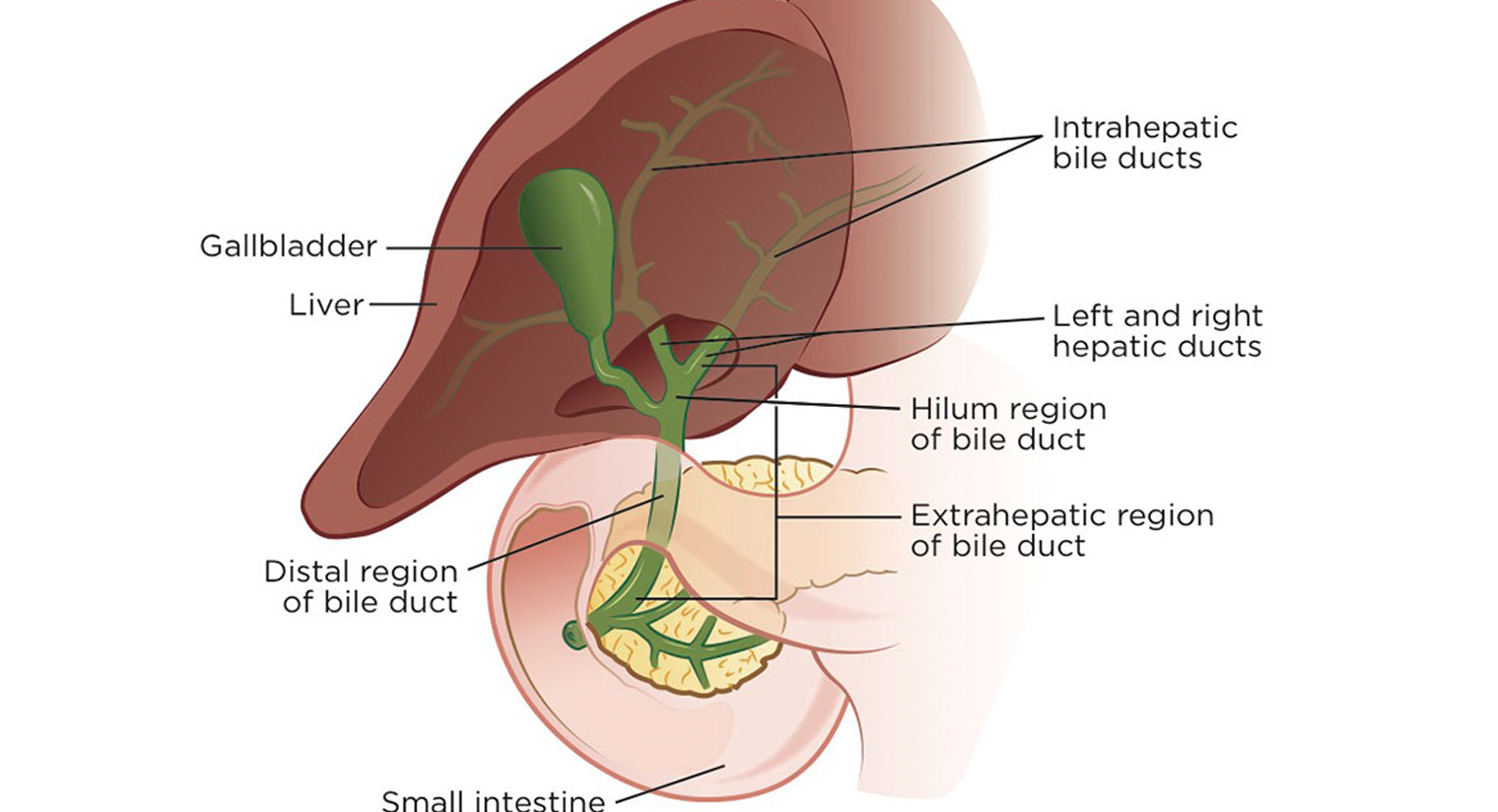
Cholangiocarcinoma is a rare cancer that starts in your bile ducts. Bile ducts are thin tubes that bring bile (a fluid that helps you digest fats) from your liver and gallbladder to your small intestine.
Cholangiocarcinoma is an aggressive cancer, which means it spreads fast. Most people receive a cholangiocarcinoma diagnosis after it’s already spread outside of their bile ducts. At this point, bile duct cancer is difficult to treat, and the prognosis (chance of recovery) is usually poor.
Experts are continually researching and developing new treatments that can slow cancer spread and improve the outlook associated with cholangiocarcinoma.
What are the types of bile duct cancer?
There are three types of cholangiocarcinoma:
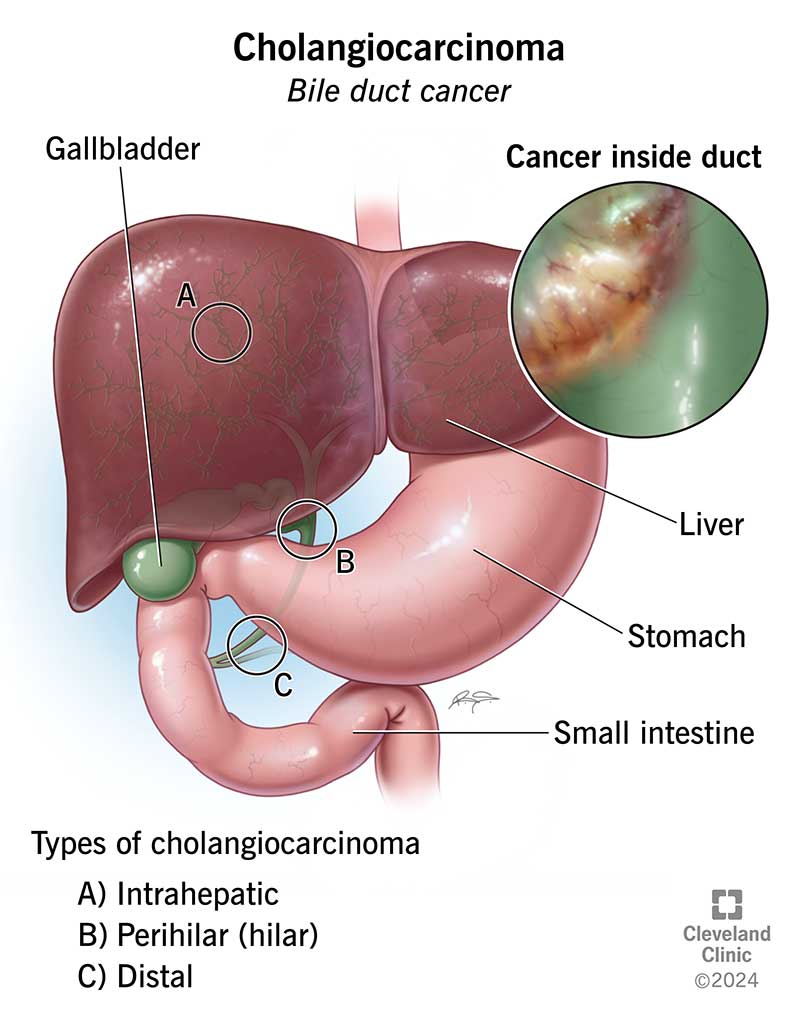
- Intrahepatic cholangiocarcinoma is bile duct cancer inside your liver.
- Perihilar (hilar) cholangiocarcinoma is bile duct cancer in your hilum. The hilum is the area just outside your liver where the smaller bile ducts from inside your liver merge to form a larger duct called the common hepatic duct. It’s the most common form of cholangiocarcinoma. Another name for perihilar cholangiocarcinoma is a Klatskin tumor.
- Distal cholangiocarcinoma is bile duct cancer that starts outside your liver, in the ducts closer to your small intestine.
Perihilar cholangiocarcinoma and distal cholangiocarcinoma are also known as extrahepatic bile duct cancers because they form outside your liver (“extra”-hepatic) instead of inside your liver (“intra”-hepatic).
How common is this condition?
Cholangiocarcinoma is rare. About 8,000 people in the United States develop this cancer each year. It’s most common in people around age 70.
Worldwide, cholangiocarcinoma is more common in Southeast Asia. Bile duct cancer is a complication of clonorchiasis, a chronic (long-term) infection associated with a Chinese liver fluke parasite.
Symptoms and Causes
What are the symptoms of cholangiocarcinoma?
Cholangiocarcinoma symptoms don’t usually start until the cancer advances and blocks a bile duct. Symptoms of bile duct cancer include:
- Abdominal pain.
- Fever.
- Fatigue.
- Itchy skin.
- Jaundice (skin and whites of eyes turn yellow).
- Dark urine.
- Light-colored or greasy stools.
- Nausea and vomiting.
- Unexplained weight loss.
Cholangiocarcinoma isn’t usually painful in the early stages. But a large tumor can cause pain that may feel concentrated in the right side of your abdomen, underneath your ribs. For some people, the pain may shift to other regions in their abdomen or back.
But this type of pain is common in many conditions, not just bile duct cancer. It’s important to see a healthcare provider to determine what’s causing unusual abdominal pain.
What causes cholangiocarcinoma?
Experts don’t know exactly what causes cholangiocarcinoma. But health conditions that cause chronic (long-term) inflammation in your bile ducts may play a role.
Ongoing damage from inflammation can cause changes in cell DNA. DNA contains the instructions that tell cells how to behave. Damaged DNA can cause problems with how cells grow and divide, creating tumors that damage tissue. These changes probably aren’t inherited (passed down from biological parents to their children). Instead, they likely happen during a person’s lifetime.
Risk factors of cholangiocarcinoma
You may be more likely to develop cholangiocarcinoma if you have:
- Structural abnormalities where your bile duct and pancreatic duct meet.
- Bile duct stones or choledochal cyst disease (bile duct cysts).
- Clonorchiasis (infection with a Chinese liver fluke parasite).
- Chronic ulcerative colitis.
- Cirrhosis of the liver.
- Hepatitis B or hepatitis C.
- Human immunodeficiency virus (HIV).
- Inflammatory bowel disease (IBD).
- Metabolic dysfunction-associated steatotic liver disease.
- Primary sclerosing cholangitis (inflammation and scarring that blocks your bile ducts).
Additional risk factors include:
- Alcohol use disorder.
- Diabetes.
- Obesity.
- Smoking.
Exposure to toxins (especially chemicals used in rubber plants or automotive factories).
Diagnosis and Tests
How is cholangiocarcinoma diagnosed?
A healthcare provider will evaluate your symptoms, review your medical history and do a physical exam.
Tests for cholangiocarcinoma may include:
- Liver function tests: These liver tests check your blood for high levels of substances, such as elevated liver enzymes, that might indicate your liver isn’t working as it should. High levels may also mean you have a bile duct blockage.
- Tumor marker tests: These tests check your blood or urine for tumor markers — substances that might mean you have cancer. High levels of carbohydrate antigen (CA) 19-9 or carcinoembryonic antigen (CEA) may be signs of bile duct cancer.
- Imaging tests: An abdominal ultrasound is usually the first imaging test you’ll need if your provider suspects bile duct cancer. You may also need a CT scan or an MRI, including a specialized MRI called magnetic resonance cholangiopancreatography (MRCP).
- Endoscopic tests: These tests use an endoscope (a thin, flexible tube with a camera) to examine your bile ducts. While you’re sedated (in a light sleep), the endoscope goes into your mouth and down to your small intestine so your provider can see your bile ducts up close. Tests include endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP).
- Percutaneous transhepatic cholangiography (PTC): A PTC is a procedure that can be used to view bile duct blockages related to cholangiocarcinoma and drain the blockage. During the procedure, your provider will deliver a contrast dye directly into your bile ducts and liver. The dye causes blockages to show up more clearly on an X-ray. They’ll place a tube into the bile duct so it can drain. A PTC is usually only for people who can’t have an ERCP.
If test results indicate cancer, your healthcare provider will perform a biopsy to confirm the diagnosis. A biopsy removes a tissue sample so it can be tested for cancer. Your provider can take samples during an ERCP or PTC by inserting a small needle through your skin.
If you do have cholangiocarcinoma, your provider may perform tests on your tissue biopsy and blood (liquid biopsy) to check for genetic changes in cancer cells (biomarkers). Cholangiocarcinoma tumors can have important biomarkers. If they’re present, you may be eligible for special cancer treatments that target these cells for destruction (targeted therapy).
How is cholangiocarcinoma staged?
Cancer staging is an important part of a bile duct cancer diagnosis. It allows your healthcare provider to determine how much cancer is in your body. Staging helps your provider plan treatment and determine your prognosis.
Staging guidelines are different for each type of cholangiocarcinoma. But in general, bile duct cancer staging looks at the size of the tumor and whether cancer has spread from the bile ducts to your:
- Blood vessels.
- Lymph vessels and lymph nodes.
- Organs near your bile ducts, like your liver or gallbladder.
- Distant organs, such as your lungs, bones or abdominal cavity.
The staging scale ranges from stage 0 to stage 4. The least advanced and most treatable is Stage 0, or carcinoma in situ. This means you have abnormal cells that could become cholangiocarcinoma, but haven’t yet. Stage 4 is the final (or most advanced) stage of cholangiocarcinoma. At this stage, the cancer is metastatic. It’s spread beyond your bile ducts to distant parts of your body.
Management and Treatment
How is cholangiocarcinoma treated?
Cholangiocarcinoma treatment depends on where it’s located and if it has spread. Surgery can treat bile duct cancers that haven’t spread. But most bile duct cancers have spread by the time they’re diagnosed.
If surgery alone won’t eliminate cholangiocarcinoma, your healthcare provider may recommend a combination of treatments to slow cancer growth or provide palliative care that relieves symptoms.
Cholangiocarcinoma treatment may include:
- Surgery: Removes all or part of your bile duct or affected organs. Surgery can also help treat a blocked duct that’s causing symptoms. Your provider may place a stent (small, hollow tube) to drain it or reroute the flow of bile past the blockage.
- Liver transplant: Replaces your liver with a donor liver. A transplant is one potential cure for early-stage perihilar cholangiocarcinoma.
- Radiation therapy: Uses radiation to kill cancer cells or shrink tumors. You may need external beam radiation therapy (EBRT), which uses a machine outside your body to direct radiation toward the tumor. Or your provider may implant tiny beads of radiation (called Y90) in the blood vessels supplying the tumor to shrink it. This is called transarterial radioembolization (TARE).
- Chemotherapy (chemo): Uses drugs to kill cancer cells or shrink tumors. Systemic chemotherapy sends the medicine through your entire body. Transarterial chemoembolization (TACE) implants tiny beads of chemo into the blood vessels near your tumor to shrink it. Hepatic artery chemo-infusion (HAI) uses a pump to inject chemo into the artery that supplies blood to your liver.
- Targeted therapy: Zeroes in on specific proteins on cancer cells. Some people with bile duct cancer have abnormal proteins that cause cells to grow out of control. Targeted therapies block the abnormal proteins that fuel cancer growth.
- Immunotherapy: Helps your body’s immune system fight cancer. In bile duct cancer, some cancer cells contain a protein that prevents immune cells from attacking. Immunotherapy disables this protein so immune cells can attack the cancer.
- Clinical trials: Studies that test the effectiveness of new cancer treatments or new combinations of existing treatments. If your cancer is too far advanced for surgical removal, your provider may recommend taking part in a clinical trial.
Prevention
How can I prevent cholangiocarcinoma?
There’s no way to prevent bile duct cancer, but you can reduce your risk by protecting your liver (and bile ducts) from inflammation. This includes:
- Protecting yourself from viruses such as hepatitis B, hepatitis C, and HIV.
- Limiting the amount of alcoholic beverages you drink.
- Maintaining a healthy body weight.
- Quitting smoking.
Outlook / Prognosis
What is the prognosis?
The outlook (prognosis) for people with cholangiocarcinoma is usually poor.
The five-year survival rate for cholangiocarcinoma that hasn’t spread outside of the bile ducts ranges from 18% to 23%. That number drops to 2% to 3% for cancer that’s spread beyond bile ducts.
Still, it’s important to remember that new cancer treatments are continually improving survival rates and the experiences of people living with cancer. Five-year survival rates reporting on statistics from previous years don’t reflect these developments.
Talk to your healthcare provider about your prognosis based on your cancer diagnosis, including the type of cholangiocarcinoma and its stage.
How curable is bile duct cancer?
Bile duct cancer is curable in the early stages if your provider can surgically remove all affected tissue. At this point, a liver transplant may also be a potential option for curing cholangiocarcinoma.
But only a small amount of bile duct cancers are curable because they’re usually not diagnosed until the cancer has already spread. At this point, it’s impossible to get rid of cholangiocarcinoma with surgery alone.
Living With
What questions should I ask my healthcare provider?
Questions to ask include:
- What type of cholangiocarcinoma do I have?
- What is the stage of the cancer?
- What treatments would you recommend?
- Do I need biomarker testing?
- Are there clinical trials I can take part in?
- What treatment side effects should I expect?
- Is there anything I can do to make treatment more effective?
- How likely is it that cholangiocarcinoma will come back after treatment?